





























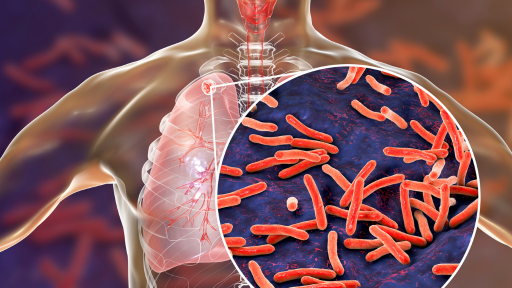
Uncover the Global TB Landscape
Join the fight against TB! Explore the challenging global TB landscape and the critical role of diagnostic testing in treatment, prevention and elimination.
Latent TB methods
Two types of latent TB tests utilize the immune response to detect TB: skin tests (tuberculin or specific TB antigens) and interferon-gamma release assays (IGRAs). The skin tests have significant drawbacks, including the requirement for two clinic visits, specialized staff training, potential reactivity to Bacillus Calmette-Guérin (BCG) vaccination leading to false positives, and only moderate sensitivity and specificity, potentially resulting in missed latent TB cases.4
In contrast, IGRAs function by identifying TB-specific effector T cells from the blood in vitro for latent TB detection. These tests are conducted in the laboratory, necessitate only one patient visit, and crucially remain unaffected by BCG vaccination.5,6
There are two different IGRAs:
- ELISPOT IGRA (the T-SPOT.TB test) - Where peripheral blood mononuclear cells (PBMCs) are isolated, washed and counted to purify them from the whole blood prior to cell stimulation.
- ELISA/CLIA IGRAs - Where the cell stimulation is performed in the whole blood.
Why T-SPOT.TB?
- High sensitivity and specificity providing accurate results5
- Maintains performance in the immunosuppressed9.13
- Low indeterminate results, few repeat tests12
The T-SPOT.TB test has three crucial steps that have recently been acknowledged by the WHO for ensuring reproducibility and mitigating the impact of pre-analytical variables.7 These steps include isolating, washing, and counting the PBMCs before the test is performed. Shifting from traditional whole blood sample testing, the T-SPOT.TB test provides precision and reliability, allowing more control in your TB infection testing.
Here's how:
- Only one standard blood collection tube is needed throughout the T-SPOT.TB process
- Isolates PBMCs from whole blood, washes and counts them:
- Isolate cells: Extract the desired cell population (PBMCs) from whole blood
- Wash cells: Enables removal of potential interfering substances from whole blood
- Count cells: Ensures the required number of cells are used to produce reportable and accurate results regardless of individual patient cell counts
- Directly visualize the results without relying on interpretations from standard curves

Explore our TB Management related solutions

Expert opinions
For World TB Day this year, we asked our experts: 'what's the most impactful action we can take today to accelerate the end of TB?'

"To accelerate the end of TB, we must focus on immediate case identification and treatment, robust contact screening, enhance detection of latent tuberculosis infection through specific advanced diagnostic tools. especially in high-risk and immunocompromised populations. With this multi-prong approach, we can break the cycle of TB transmission and move closer to global TB elimination"
Juzar Ali
MD, Professor (Emeritus) of Medicine at Louisiana State University Health Sciences Center

"The biggest challenge is convincing healthcare providers of the necessity of testing. Especially in patients with HIV or under immunosuppressive therapy, who are at high risk of developing active TB, early detection is key: If you can diagnose and treat LTBI before progressing into active disease, it's much easier, especially if you're comparing it to treating extensively drug-resistant tuberculosis. Early detection and intervention are key to preventing active TB disease and ultimately accelerate the end of TB."
Dr Martin Obermeier
Lab Manager at the Medical Centre for Infectious Diseases in Berlin (MIB)

"TB is widespread in our country, affecting both urban and rural areas. Early detection of all forms of TB is crucial for controlling its spread. Identifying latent TB is essential, as many are unaware, they have it. Diagnosing extra-pulmonary TB, often missed by conventional methods, is critical. We've seen many unexpected cases linked to it. Comorbidities like diabetes or HIV complicate TB cases and require immediate identification. This World TB Day, I hope decision-makers will prioritize early detection and broader use of diagnostic tools to help end TB."
Dr Juliani Dewi, SpPK
Clinical Pathologist Lab Director, Rampal Diagnostika, Indonesia
Featured webinars




Patient stories
Behind every tuberculosis statistic is a human story. The fight against TB is not just about numbers; it's about people - their struggles, resilience, and triumphs.
Kelly
Kelly is a physician and has treated patients with TB. Being a TB patient, however, was new territory for him. One of the most difficult parts of the process was the impact on his family, friends and patients, who were forced to endure months of treatment due to their contact with him. He now brings a new understanding to his practice and works tirelessly to educate others, especially those in the healthcare community.

Taylor
Taylor is a community health worker. Originally from the Philippines, Taylor had latent tuberculosis (LTBI) and then contracted HIV. This caused her LTBI to become active, and she became very sick. After undergoing many months of treatment, Taylor recovered from TB and now works to educate others, particularly those in the LGBTQ community.
Kahyr
Khayr is a North Dakota resident and a successful hotel manager. He spent time living in Somalia as a college student, where he likely contracted multidrug-resistant (MDR) TB. Khayr was told that his chance of survival was 50%. After a long battle, he recovered and now works with We are TB, the survivor advocacy organization.
Blogs




References
- World Health Organization. The End TB Strategy. Geneva; 2014. https://www.who.int/teams/global-tuberculosisprogramme/theend-tb-strategy. Accessed: 2-AUG-23
- Global tuberculosis report 2024. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO.
- World Health Organization. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management.
- Schluger NW, Burzynski J. Recent advances in testing for latentTB.Chest. 2010 Dec; 138(6): 1456–63.
- Oxford Immunotec T-SPOT.TB Package Insert PI-TB-IVD-UK-v7. Abingdon, UK. September 2024.
- QuantiFERON®-TB Gold Plus ELISA Kit Instructions for Use. L1123669_R3_IVDr_QF_ELISA_ROW_0323_FINAL. March 2023.
- World Health Organization. WHO operational handbook on tuberculosis. October 1, 2022.
- Banaei N, Gaur RL, Pai M. Interferon gamma release assays for latent tuberculosis: what are the sources of variability? Journal of clinical microbiology. 2016; 54(4): 845–850.
- Wong SH, Gao Q, Tsoi KK, Wu WK, Tam LS, Lee N, Chan FK, Wu JC, Sung JJ, Ng SC. Effect of immunosuppressive therapy on interferon γ release assay for latent tuberculosis screening in patients with autoimmune diseases: a systematic review and meta-analysis. Thorax. 2016 Jan.
- Bèlard, et al. Prednisolone treatment affects the performance of the QuantiFERON gold in-tube test and the tuberculin skin test in patients with autoimmune disorders screened for latent tuberculosis infection. Inflammatory Bowel Diseases, Volume 17, Issue 11, 1 November 2011, Pages 2340–2349.
- Komiya K, Ariga H, Nagai H, et al. Impact of Peripheral Lymphocyte Count on the Sensitivity of 2 IFN-γ Release Assays, QFT-G and ELISPOT, in Patients with Pulmonary Tuberculosis. Intern Med. 2010; 49(17): 1849–55.
- Rego K, et al. Utility of the T-SPOT®.TB test's borderline category to increase test resolution for results around the cut-off point. Tuberculosis. 2018; 108:178 185.doi:10.1016/j.tube.2017.12.005.
- Clark SA, Martin SL, Pozniak A, et al. Tuberculosis antigenspecific immune responses can be detected using enzymelinked immunospot technology in human immunodeficiency virus (HIV)-1 patients with advanced disease. Clin Exp Immunol. 2007; 150(2):238–244.
For in vitro diagnostic use. This product is only available where licensed in accordance with the law. Please contact your local representative for availability. Revvity Inc. does not endorse or make recommendations with respect to research, medication, or treatments. All information presented is for informational purposes only and is not intended as medical advice. For country specific recommendations, please consult your local health care professionals.

How can we help you?
We are here to answer your questions.